

Maternal Mortality in the US
Why the United States has the highest maternal mortality rates of all wealthy countries
The U.S. is known for its premiere medical care. People come here from all over the world for state of the art healthcare. After all we spend 17% of our GDP on healthcare. However, you may not know that it is safer to have a baby in many European or South American countries than it is in the U.S. The maternal mortality rate in the U.S. is more than ten times the estimated rates of other developed countries.
36% of counties in the U.S. are considered Maternal Care Deserts and over 50% of counties have no hospital services for deliveries. The reasons are complicated. One reson is that hospitals cannot afford to offer obstetric services with the poor reimbursement rates offered by insurance companies and Medicaid.
A Maternal Care Desert is defined as a "county where there is a lack of maternity care resources". Of the 44 counties in Idaho, over half are considered "Maternal Care Deserts"; Bonner and Boundary County being in this group.
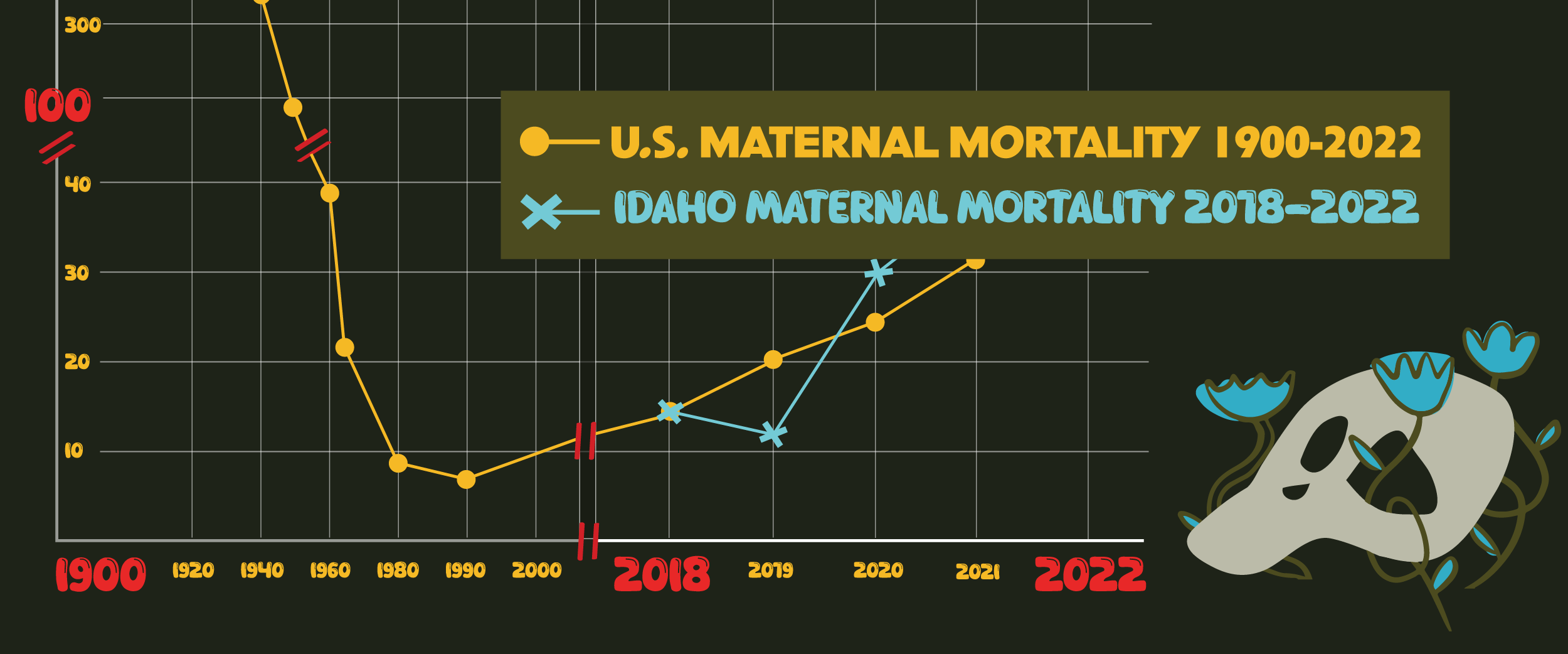
The lowest maternal mortality rate in the U.S. was in 1980-1990, with 8 maternal deaths/100,000 live births. In 2018 it was 17.4 maternal deaths/100,000, and by 2021 it was over 32/100,000 live births. There are countries in Europe with a 0 -1 maternal deaths/100,000 live births. Why is there such a difference? What is the explanation for the increase in the U.S. rates and what can be done?
It is not a coincidence that legislation in our state has led to an exodus of OB-GYN's and Maternal Fetal Medicine Specialists. Almost 25% of our OB-GYN's have left, fearing criminalization when offering evidence-based medicine. 64% of OB-GYN's feel that the Supreme Court ruling has worsened maternal outcomes.
THE STATE OF MATERNAL HEALTH IN THE U.S. IS DIRE AND DEMANDS IMMEDIATE ACTION

Are You Okay?
Karli Fairbanks
The state of maternal health in the US is dire
Why would anyone think that pregnancy or having a baby is now a dire subject? What usually would carry promise and excitement has a cloud over it. News accounts suggest we should be asking questions and giving new Idaho legislative decisions a lot more gravitas. Now, as women and their partners and families discuss what the new laws in their home state mean for them, they might consider moving elsewhere.
We hope our examination of maternal health complications helps illuminate the intricacy of what Maternal Mortality is, and what the underlying data actually means. We also address the added ramifications when state officials insert themselves in the exam room, which further complicates this already difficult subject. Maternal healthcare concerns discussed with a medical provider aren’t so clear anymore. Let’s look at why.
Oh, those darn statistics.
We remember all too well the horrific numbers and variability in causes of deaths from COVID-19. Each state’s department of health had its own way of collecting data about COVID cases, including ages or age ranges, sex, hospitalizations, vaccinations, deaths, etc. This left national agencies of health and researchers in a quandary on how best to compare and contrast diversely documented information, and then report it back to the public.
Similarly, collecting Maternal Mortality statistics is not always as straightforward as one may think. Recording practices vary from state to state, and with who is filling in the information. A medical provider who completes a death certificate may do so quite differently than other staff. As a result, a key piece of information can easily be lost in the mix of data, such as: “was this death related to the person’s status of being pregnant?”
Here’s an example when a question is written poorly or recorded wrongly on a death certificate, and data becomes vague and alters interpretations of it. A checkbox was added to a death certificate asking “was the person pregnant within the last year”; the resulting study indicated that maternal mortality rates increased. Sometimes this box would be checked in error for an older person. Subsequently, having added a checkbox for age still didn’t fix this death certificate question, or how the data was reported for official death records.
Another example of a problem with death certificates is when the cause of death is noted as “high blood pressure.” The diagnosis of high blood pressure would need to be associated with a person's status of pregnancy or recent pregnancy for Maternal Mortality reporting purposes. It’s far more difficult to collect data about a person’s death — whether it was maternal-caused or pregnancy-associated — if the appropriate pregnancy box is not checked.
Race and socio-economic status play a role in maternal mortality.
Many would be surprised to know that a black woman with a PhD has a higher rate of death during pregnancy than a white woman who is in high school. Black pregnant women, in particular, suffer the worst maternal health disparities and have the highest rate of maternal death. This is largely due to racial and socio-economic inequities, including, access to quality health care, nutritious food, safe housing and home or neighborhood environment, employment opportunities, financial security, and more. How does a society start to level this uneven playing field and address the systemic, structural, and social determinants of health?
Consistency and precision matter in defining the cause of death during pregnancy.
Compounding disparities in diagnoses is data collection terminology, such as: “year of pregnancy being measured”. There is a specific definition of time that statisticians use to collect information about maternal mortality. However, the American College of Obstetricians and Gynecologists (ACOG) collects data differently than the Centers of Disease Control and Prevention (CDC). For example, a report indicated deaths of pregnant persons “in the hospital” have decreased – suggesting improved care during hospitalization. However, continued rising death rates of pregnant people and new mothers point to the vulnerable times when maternal deaths occur outside the labor and delivery unit. In order to achieve a more accurate measurement of maternal mortality, we need to identify these unique situations that led to death during a woman’s pregnancy, and address the causes, regardless of when in the “year of pregnancy” the death occurred.
The U.S. maternal mortality rate is more than ten times that of other developed countries.
Regardless of the numbers, the significant fact here is that the U.S. – the country that spends the most on healthcare (18% GDP) of all developed countries – has the highest maternal mortality of ALL developed countries. In 2020, the average maternal mortality of all high-income countries was 12/100,000, whereas in the U.S. it was almost 24/100,000 and is climbing. Compare these numbers to some European countries that have rates of 0-3/100,000. In contrast, the U.S. had its lowest rate of maternal mortality from 1980 through 1990. Clearly, we can do better!
The most common contributors to maternal mortality in the U.S. include several conditions. Some may be surprised to learn that mental health is the leading cause. Other reasons are hemorrhage, cardiac issues, infection, blood clots, high blood pressure related to pregnancy, amniotic fluid embolism, injury, cerebrovascular accidents, cancer, endocrine/metabolic disorders, and pulmonary conditions.
It’s important to know that almost all maternal deaths are preventable with adequate screening, and prenatal and postpartum care. There are several other interventions that also reduce maternal deaths such as avoiding unintended pregnancies, extended postpartum care, and increasing strong social support systems for our pregnant women. However, there is far more information to be gleaned from the data and to be studied. Does the U.S. have the commitment and the money to find out?

As we consider these national questions, Idaho laws have complicated and endangered pregnant women’s outcomes.
Closer to home, Idaho has passed laws that essentially ban all abortions in the state (except for the trinity: “rape, incest and ‘the life of the mother’”). We can expect maternal mortality to increase in our state as it has in other states where restrictive laws against women’s reproductive agency have been passed.
This legislation has precipitated an exodus of obstetricians/gynecologists (OB-GYNs) from Idaho (22% since this legislation passed) due to the criminalization of evidence-based care. It has also “chilled” recruitment of not just OB-GYNs, but other physician specialties (and medical students) from considering Idaho as a place to practice medicine. Idaho was a medically underserved state before the 2022 legislation session. It’s worse now. Advertising our beautiful state, outdoor life, and rural backdrop can not correct for the decisions made in our Capital Building. It is dangerous to be pregnant in Idaho.
The Good News: Idaho expanded Postpartum Medicaid coverage.
The 2024 Idaho legislature extended Postpartum Medicaid to a full 12 months after birth. Before this law was passed, Idaho covered only two months of postpartum healthcare. As a result, many women would drop out of the healthcare system, some before they had their single visit after their baby was born. This critical visit is one of the highest “no-shows” during the pregnancy care bundle. We were cutting off women’s access to healthcare at the point when data shows a strong and life-saving need for medical and social support services. We were also making it harder for new mothers to obtain effective birth control so they could heal from their pregnancy and birth, and focus on their new baby.
Then, Idaho took a step backward with changes to a Maternal Mortality Review Committee.
Measuring maternal deaths in Idaho should not be a political ping-pong or budgetary issue. The Idaho legislature let the Maternal Mortality Review Committee (MMRC) sunset as of July 1, 2023 – a federally funded multidisciplinary committee that analyzed maternal deaths and made recommendations to all medical providers in Idaho. This Committee was consistent with 49 other states, to ensure that the U.S. and states were comparing apples to apples when determining maternal mortality rates and causes.
Eventually, Idaho will begin collecting Maternal Mortality data again… but not the right data, the right way, or by the right people. During the 2024 Idaho legislative session, Idaho passed what they “call” the MMRC (which it isn’t). This new committee is administered by a different government agency and is now tasked with comparing different data sets, collected and analyzed by a different group of medical professionals. And this committee is formed by a group of physicians only (not the multi-disciplinary team of the MMRC).
The importance of a multidisciplinary team is that maternal deaths are a complex event; an event that requires all types of medical professionals to collaborate on causality, and determine the best intervention by everyone involved in the care of the pregnant woman. And, the new committee does not use federal funds. It remains to be seen if they are going to be effective when reviewing and making recommendations to Idaho medical providers in order to address maternal mortality in our state. We are paying attention.

Increasing rates of maternal death is not acceptable.
We need to turn this alarming and tragic trajectory around. Here are a few ways you can make a difference:
Share what you learned about maternal mortality with your family, friends, and neighbors. Host conversations about reproductive rights and care in your home or community. Plan a dinner, start a book club, invite a speaker.
Write, call, or speak with your Idaho legislator. Request they reinstate the Maternal Mortality Review Committee (MMRC) as it was formally organized with federal funding prior to July 1, 2023. legislature.idaho.gov/legislators/whosmylegislator
Dialog with candidates and elected officials in person, via email, or over the phone. Tell them you support medically-based legislation that attracts physicians and medical students to work in Idaho (and other care deserts). legislature.idaho.gov/legislators/contactlegislators
Vote—every single election—like your rights depend on it. Seek out lawmakers who support women, their healthcare needs, and reproductive and bodily autonomy rights. vote.idaho.gov
Support nonprofits already doing the work to effect change. Volunteer, donate, fundraise.
Join The Pro-Voice Project today to change the conversation about women’s reproductive rights! Let your voice be heard. Speak to what matters to you. theprovoiceproject.com
Maternal Mortality News, Studies & Stats



The Boards
-
![]()
Your Body Is a Battleground
Legal barriers to reproductive healthcare over time.
-
![]()
Women Weaving Community
Historical contributions of women to our community.
-
![]()
Maternal Mortality in the US
A look at maternal mortality rates and contributing factors.
-
![]()
Shame, Stigma, Silence
The moral and social dimensions of gynecology.
-
![]()
Undervalued, Under-treated, Under-Studied
How we systemically undervalue women's healthcare.
-
![]()
(CO)Operation
How different care options play out in one's life.
-
![]()
Map of Gynecologia
The previously uncharted wilderness of Women’s healthcare.
-
![]()
The Future
What do you want to see for the future in the state of Idaho?
-
![]()
BGH Birth Stories
Personal accounts and birth stories at Bonner General Hospital.








RESOURCES
FOOTNOTES
Data and research often presume cisgender identities and may not systematically account for people who are transgender and non-binary. The language used attempts to be as inclusive as possible while acknowledging that the data we are citing uses gender labels that we cannot change without misrepresenting the data.